












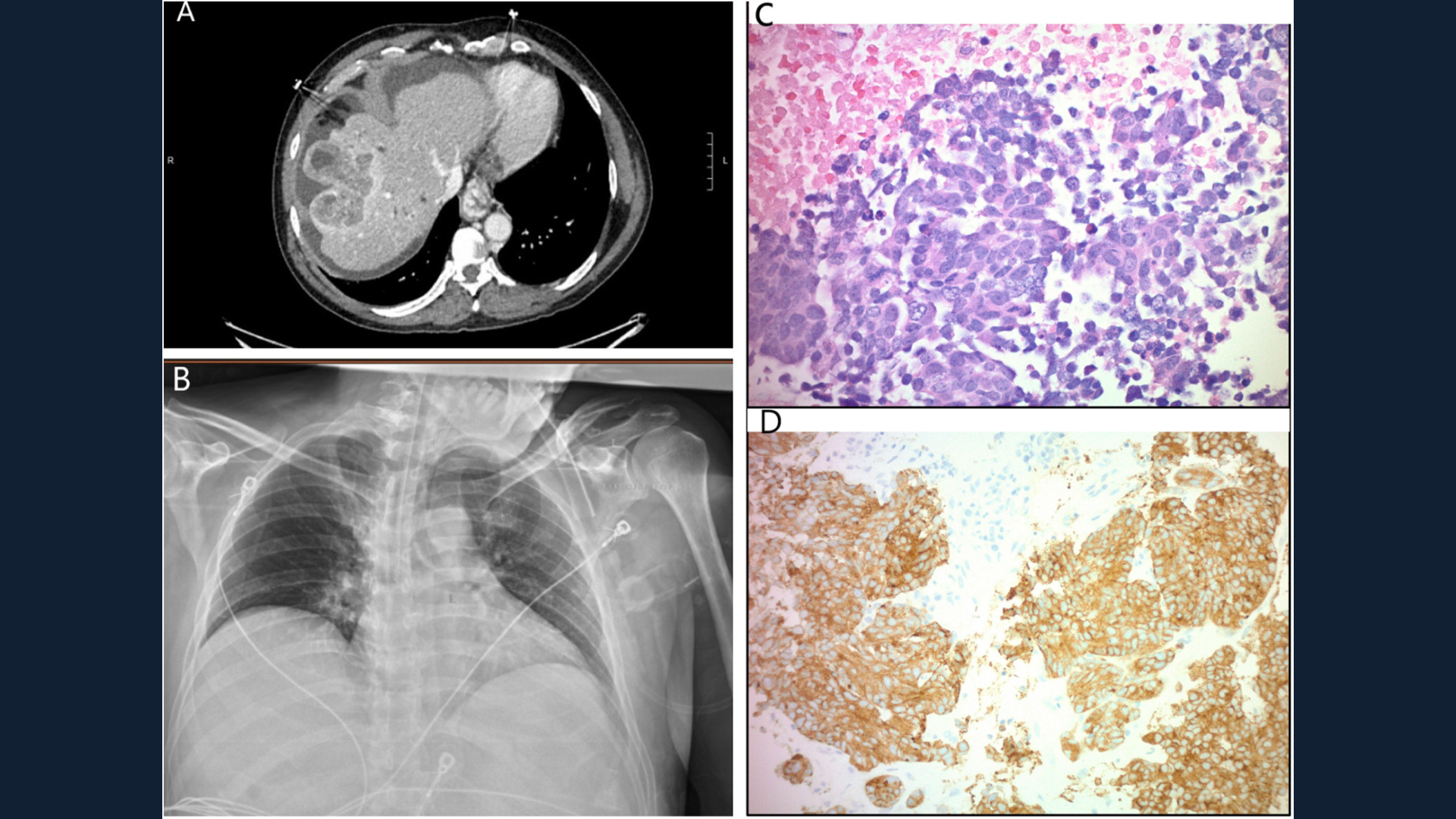
Gastroenterology image challenge: A 52-year-old Hispanic man with obesity (body mass index 30 kg/m2) and hypertension on amlodipine presented with abdominal pain, hematemesis and melena. The patient reported routine alcohol consumption of 2-3 beers per day for 30 years, but was never a smoker. He denied any personal or family history of chronic liver disease, cirrhosis or malignancy. On examination, jaundice, scleral icterus and abdominal distension without tenderness were present. Laboratory studies revealed increased aspartate transaminase of 151 U/L, alanine aminotransferases of 40 U/L, alkaline phosphatase of 729 U/L, total bilirubin of 4.5 mg/dL and prothrombin international normalized ratio of 1.4. The albumin was decreased at 2.7 g/dL and platelet count were within the normal range at 239,000 mm3. A dual-phase computed tomography (CT) scan of the abdomen with intravenous contrast revealed a large heterogeneous, peripherally and arterial hyperenhancing mass (8.4 × 4 .7 cm) in the right hepatic lobe with similar appearing smaller satellite lesions (Figure A).
Enlarged retroperitoneal lymph nodes and ascites were present with edema of the ascending colon secondary to portal hypertensive colopathy. The imaging characteristics of the pancreas, spleen, kidneys and adrenal glands were normal. A posterior–anterior and lateral chest radiograph (Figure B) and CT scan of the chest were normal, with no perihilar lymphadenopathy. Carcinoembryonic antigen was mildly elevated 3.9 ng/mL (reference value, ≤2.5 ng/mL); however, other tumor markers were normal. Ascites was serous with an albumin of <1.0 g/dL, protein of 1.4 g/dL, serum–ascites albumin gradient of >1.1 g/dL, and absolute neutrophil count of 20 cells. Fluid cytology was negative for malignant cells.
A positron emission tomography–CT scan from the skull base to mid-thigh revealed an ill-defined hepatic dome hypermetabolic mass with multiple smaller foci of uptake along the hepatic dome, suggestive of extrahepatic malignant implants, splenomegaly and moderate to large volume ascites. No mediastinal, hilar, or axillary lymphadenopathy, pulmonary nodules or effusion were present. Although the patient had risk factors for both nonalcoholic and alcohol-related liver disease, the diagnosis of cirrhosis with portal hypertension as opposed to tumor-related portal hypertension could not be discerned. An esophagogastroduodenoscopy showed 4 columns of grade II varices in the lower one-third of the esophagus (4 bands were successfully placed), moderate portal hypertensive gastropathy in the entire examined stomach, and a normal examined duodenum. Magnetic resonance imaging of the brain showed no evidence of metastatic disease. A biopsy of the liver mass demonstrated poorly differentiated carcinoma with tumor necrosis, abundant apoptotic bodies and tumor cells showing a high nuclear to cytoplasmic ratio (original magnification ×400) (Figure C); strong and diffuse immunohistochemically reactive staining was noted for synaptophysin (original magnification ×200) (Figure D), and CD56.
How would you diagnose and treat this patient?
