











Gastroenterology image challenge: A 75-year-old man presented with a one-month history of mild abdominal pain and cramping, associated with weight loss (3 kg). He denied any nausea, vomiting, chills, diarrhea or hematochezia. The patient reported no trauma. He had a history of ampullary adenocarcinoma treated with pancreaticoduodenectomy two years earlier. The postoperative course was marked by hemorrhagic shock owing to a splenic artery pseudoaneurysm that was successfully treated by trans-arterial embolization.
On physical examination, the patient was afebrile and had normal vital signs. He had a slight tender abdomen on palpation. Blood tests revealed a C-reactive protein level of 20.2 mg/L (reference value, <3.5 mg/L) and a white blood cell count of 3670/mm3 with 87% neutrophils. Other laboratory tests were unremarkable.
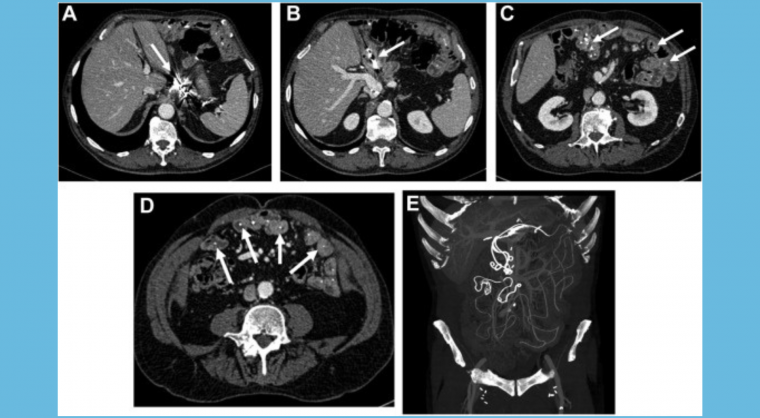
A contrast-enhanced computed tomography (CT) scan showed a status post embolization of the splenic artery with hyperattenuating embolic material (Figure A) and long thin hyperattenuating foreign bodies in the small bowel lumen (Figure B–D; the entire CT scan is provided as supplemental material) that were better assessed on a coronal maximum intensity projection view (Figure E). The small bowel wall was normal. There was no sign of bowel perforation, no fluid collection, and no sign of active or recent bleeding. The colon was normal. The pancreaticojejunal anastomosis was unremarkable. There was no evidence of tumor recurrence.
What is the correct diagnosis?