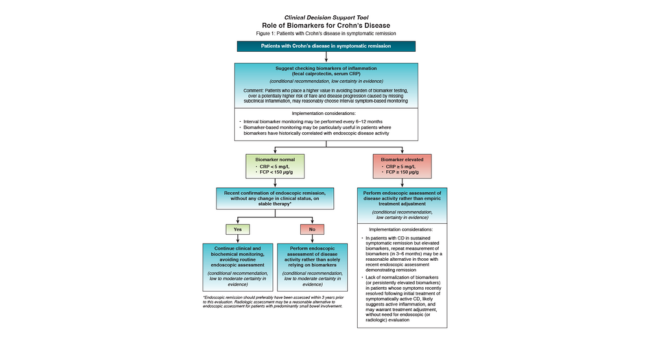
"Patients’ symptoms do not always match endoscopic findings, so biomarkers are a useful tool to understand and monitor the status of inflammation and guide decision making in patients with Crohn's disease.”
“Based on this guideline, biomarkers are no longer considered experimental and should be an integral part of IBD care. This is a win for Crohn’s disease patients. Biomarkers are usually easier to obtain, less invasive, more cost-effective than frequent colonoscopies and can be assessed more frequently for tighter disease control and better long-term outcomes in Crohn’s disease.”