











Through the end of the year, we’re bringing back some of the best articles from the retired AGA Journals blog, Digest This. Learn about a patient with gastric rotation in this article from May 2016.
Researchers reported a case of gastric rotation, with inversion of the greater and lesser curvatures along the long axis of the stomach, in the May issue of Gastroenterology.
Fady G. Haddad et al describe a 56-year-old woman with history of peptic ulcer disease, diverticulosis, hypertension and hypothyroidism who presented with acute post-prandial epigastric pain. She reported that milder similar episodes had occurred over the last few months.
A computed tomography scan of the abdomen showed a type II paraesophageal hiatal hernia, and a large part of the stomach was noted in the chest cavity. The patient was able to eat but had transient shortness of breath after meals. A chest film revealed a retrocardiac air-fluid level, without signs of obstruction.
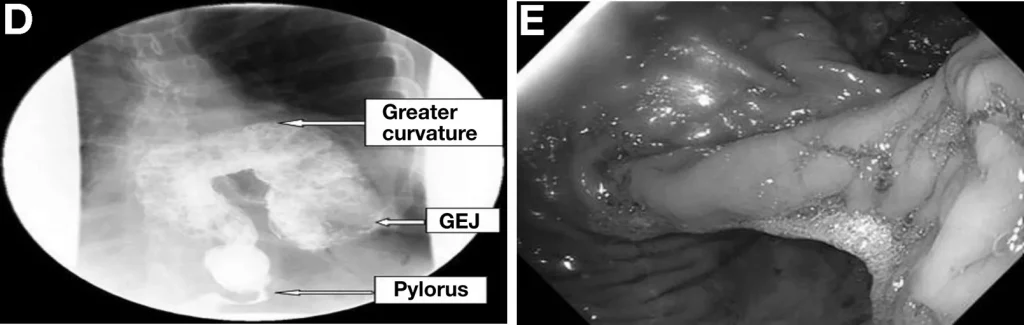
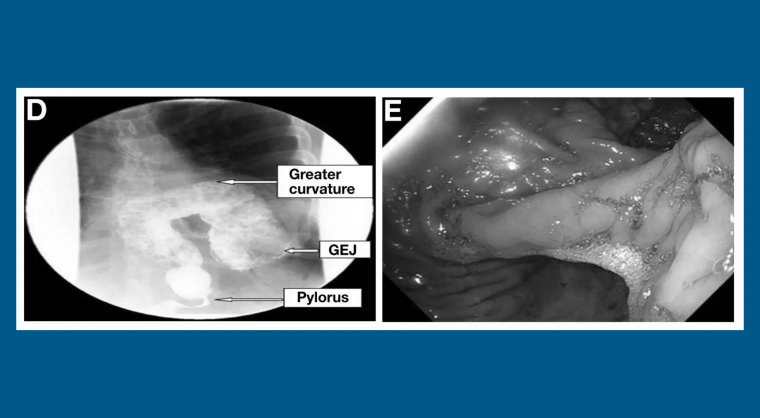
Haddad et al performed a barium study, which revealed a gastric organoaxial rotation, suggested by inversion of the greater and lesser curvatures along the long axis of the stomach (figure, left panel). Barium traversed freely to duodenum and the stomach was not distended, confirming the absence of complete volvulus.
The twisted stomach could be seen during an upper endoscopy examination (figure, right panel). The patient underwent laparoscopic reduction of the hernia with repositioning of the stomach in the abdominal cavity and gastropexy.
The authors explained that organoaxial rotation occurs when the the greater curvature of the stomach is displaced superiorly and the lesser curvature located more caudally.
A redundant paraeophageal hernia is often a predisposing factor.
Commonly, the rotation of the stomach is less than 180°, leading to a partial volvulus, in which ingested contrast material can pass through the stomach into the duodenum. Complete volvulus occurs when the twist is more than 180°.
Intermittent gastric volvulus, such as in this patient, who presented with chronic intermittent abdominal pain, can be difficult to identify, because there there are no clinical or radiologic signs during asymptomatic periods.
Patients with gastric volvulus present with gastric outlet obstruction symptoms.
A twisted stomach can have life-threatening consequences, including bowel ischemia and infarction.
Haddad et al state that it is therefore important to be aware of this disorder to avoid delays in diagnosis and complications; mortality can reach 50 percent. Treatment involves reduction of the volvulus, gastropexy and treatment of predisposing factors.

Kristine Novak, MD
Dr. Novak is a science writer and editor based in San Francisco. She has extensive experience covering gastroenterology, hepatology, immunology, oncology, clinical and biotechnology research discoveries.