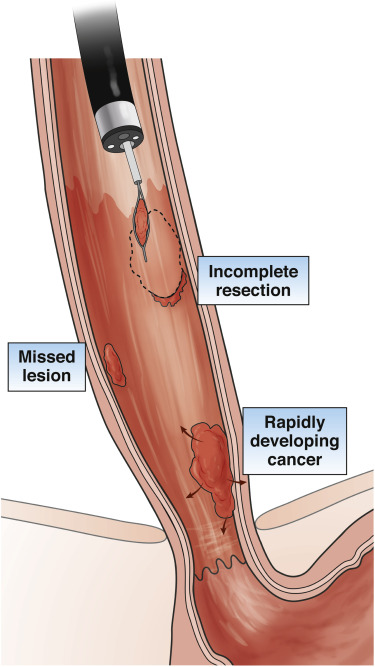
Emerging technologies may significantly alter how we perform endoscopy and serve as adjunctive approaches to impact key quality measures in Barrett’s esophagus (BE) patients including neoplasia detection rate (NDR)/dysplasia detection rate (DDR) and post-endoscopy esophageal adenocarcinoma (PEEC) rates. However, in the short term, improving upper endoscopy quality will rely on well-trained and vigilant endoscopists rather than technology enhancements. The practice of high-quality upper endoscopy is critically important to the success of any BE screening or surveillance program designed to reduce the incidence and mortality associated with PEEC and esophageal adenocarcinoma (EAC).
My AGA
AGA Journals
AGA University
AGA Research Foundation
AGA Job Board
My AGA
AGA Journals
AGA University
AGA Research Foundation
AGA Job Board
- Clinical Guidance
-
- Journals &
-
-

Male doctor reading medical record while sitting at desk. Confident healthcare worker is working in his office. He is wearing lab coat in clinic.
-
-
- Meetings &
-
-

Speaker giving a talk in conference hall at business event. Audience at the conference hall. Business and Entrepreneurship concept.
-
-
- Membership
-
-

High angle shot of a team of doctors using a digital tablet together
-
-
- Practice Resources
-
-

a medical salesman or administrator is sitting with a female doctor and running through a presentation . He is explaining something and referring to the computer screen in front of them on the desk.
-
-
- Research & Awards
-
-

Shot of a female scientist in a laboratory working with a microscope.
-
-
- Fellows & Early Career
-
-

Shot of a diverse team of doctors having a discussion
-
-