1. Care with palliative care principles should be provided to any patient with advanced serious chronic illness or life-limiting illness such as cirrhosis, irrespective of transplant candidacy; this care should be based on needs assessment instead of prognosis alone, delivered concurrently with curative or life-prolonging treatments, and tailored to stage of disease.
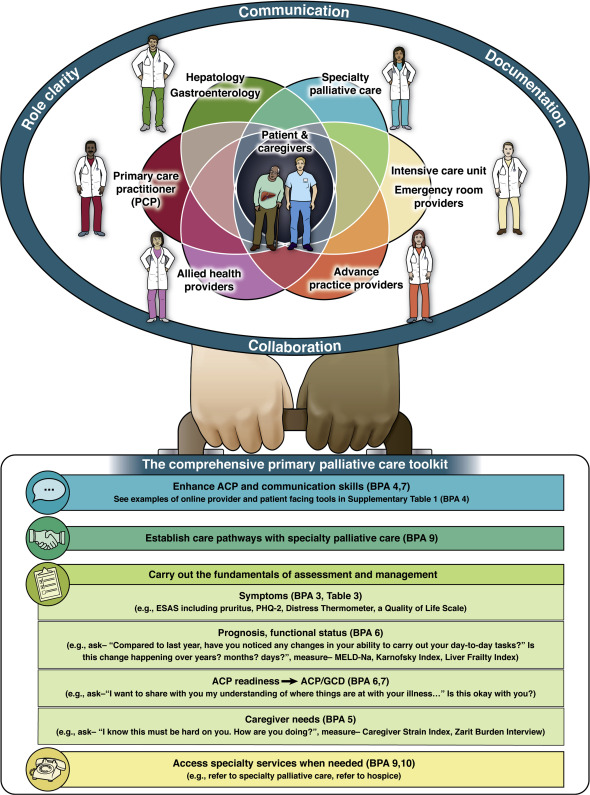
2. Care inclusive of palliative care principles may be delivered by health care providers from any specialty within any health care setting.
3. Providers caring for persons with cirrhosis should assess for the presence and severity of symptoms within physical, psychological, social and spiritual domains related to their liver disease, its treatment and prognosis.
4. Across the spectrum of cirrhosis, excellence in communication is integral to high-quality advance care planning, goals of care conversations, and the cultivation of prognostic awareness with patients and caregivers.
5. Routine care for patients with cirrhosis, and particularly those with decompensated disease, should include assessment of caregiver support and screening for caregiver needs.
6. Prognosis should be evaluated by gastroenterology/hepatology providers during routine care visits and at sentinel events.
7. Goals of care discussions in patients with cirrhosis should be repeated at sentinel events including hospital or intensive care admission, before initiation of life-supporting therapies, before surgery, on new onset of cirrhosis-related complications, and after determination of transplant eligibility.
8. Because lack of time is one of the major barriers to administering palliative care, health care providers should consider how they can optimize efficiencies in palliative care delivery (identifying local billing codes, prescreening surveys carried out by ancillary staff, development of multidisciplinary teams).
9. Dedicated specialist palliative care services are often a limited resource. As such, health care providers should work together with local specialist palliative care teams to establish clear triggers and pathways for referral.
10. Health care providers caring for patients with cirrhosis should provide timely referral to hospice for patients who have comfort-oriented goals and prognosis of 6 months or less.