1. Pancreatic necrosis is associated with substantial morbidity and mortality and optimal management requires a multidisciplinary approach, including gastroenterologists, surgeons, interventional radiologists, and specialists in critical care medicine, infectious disease, and nutrition. In situations where clinical expertise may be limited, consideration should be given to transferring patients with significant pancreatic necrosis to an appropriate tertiary-care center.
2. Antimicrobial therapy is best indicated for culture-proven infection in pancreatic necrosis or when infection is strongly suspected (ie, gas in the collection, bacteremia, sepsis, or clinical deterioration). Routine use of prophylactic antibiotics to prevent infection of sterile necrosis is not recommended.
3. When infected necrosis is suspected, broad-spectrum intravenous antibiotics with ability to penetrate pancreatic necrosis should be favored (eg, carbapenems, quinolones, and metronidazole). Routine use of antifungal agents is not recommended. Computed tomography-guided fine-needle aspiration for Gram stain and cultures is unnecessary in the majority of cases.
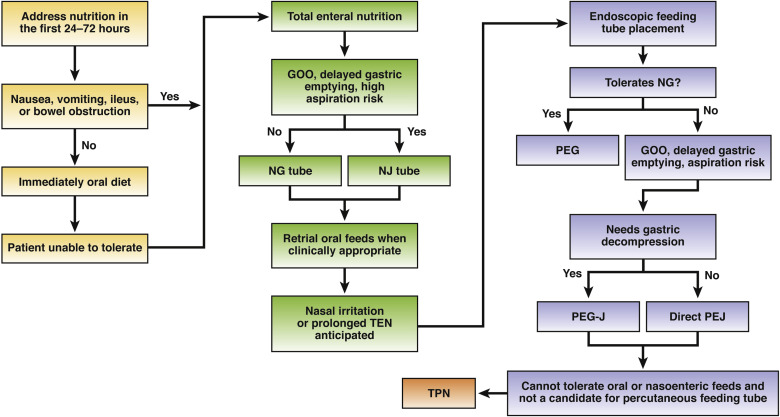
4. In patients with pancreatic necrosis, enteral feeding should be initiated early to decrease the risk of infected necrosis. A trial of oral nutrition is recommended immediately in patients in whom there is absence of nausea and vomiting and no signs of severe ileus or gastrointestinal luminal obstruction. When oral nutrition is not feasible, enteral nutrition by either nasogastric/duodenal or nasojejunal tube should be initiated as soon as possible. Total parenteral nutrition should be considered only in cases where oral or enteral feeds are not feasible or tolerated.
5. Drainage and/or debridement of pancreatic necrosis is indicated in patients with infected necrosis. Drainage and/or debridement may be required in patients with sterile pancreatic necrosis and persistent unwellness marked by abdominal pain, nausea, vomiting, and nutritional failure or with associated complications, including gastrointestinal luminal obstruction; biliary obstruction; recurrent acute pancreatitis; fistulas; or persistent systemic inflammatory response syndrome.
6. Pancreatic debridement should be avoided in the early, acute period (first 2 weeks), as it has been associated with increased morbidity and mortality. Debridement should be optimally delayed for 4 weeks and performed earlier only when there is an organized collection and a strong indication.
7. Percutaneous drainage and transmural endoscopic drainage are both appropriate first-line, nonsurgical approaches in managing patients with walled-off pancreatic necrosis (WON). Endoscopic therapy through transmural drainage of WON may be preferred, as it avoids the risk of forming a pancreatocutaneous fistula.
8. Percutaneous drainage of pancreatic necrosis should be considered in patients with infected or symptomatic necrotic collections in the early, acute period (<2 weeks), and in those with WON who are too ill to undergo endoscopic or surgical intervention. Percutaneous drainage should be strongly considered as an adjunct to endoscopic drainage for WON with deep extension into the paracolic gutters and pelvis or for salvage therapy after endoscopic or surgical debridement with residual necrosis burden.
9. Self-expanding metal stents in the form of lumen-apposing metal stents appear to be superior to plastic stents for endoscopic transmural drainage of necrosis.
10. The use of direct endoscopic necrosectomy should be reserved for those patients with limited necrosis who do not adequately respond to endoscopic transmural drainage using large-bore, self-expanding metal stents/lumen-apposing metal stents alone or plastic stents combined with irrigation. Direct endoscopic necrosectomy is a therapeutic option in patients with large amounts of infected necrosis, but should be performed at referral centers with the necessary endoscopic expertise and interventional radiology and surgical backup.
11. Minimally invasive operative approaches to the debridement of acute necrotizing pancreatitis are preferred to open surgical necrosectomy when possible, given lower morbidity.
12. Multiple minimally invasive surgical techniques are feasible and effective, including videoscopic-assisted retroperitoneal debridement, laparoscopic transgastric debridement, and open transgastric debridement. Selection of approach is best determined by pattern of disease, physiology of the patient, experience and expertise of the multidisciplinary team, and available resources.
13. Open operative debridement maintains a role in the modern management of acute necrotizing pancreatitis in cases not amenable to less invasive endoscopic and/or surgical procedures.
14. For patients with disconnected left pancreatic remnant after acute necrotizing mid-body necrosis, definitive surgical management with distal pancreatectomy should be undertaken in patients with reasonable operative candidacy. Insufficient evidence exists to support the management of the disconnected left pancreatic remnant with long-term transenteric endoscopic stenting.
15. A step-up approach consisting of percutaneous drainage or endoscopic transmural drainage using either plastic stents and irrigation or self-expanding metal stents/lumen-apposing metal stents alone, followed by direct endoscopic necrosectomy, and then surgical debridement is reasonable, although approaches may vary based on the available clinical expertise.