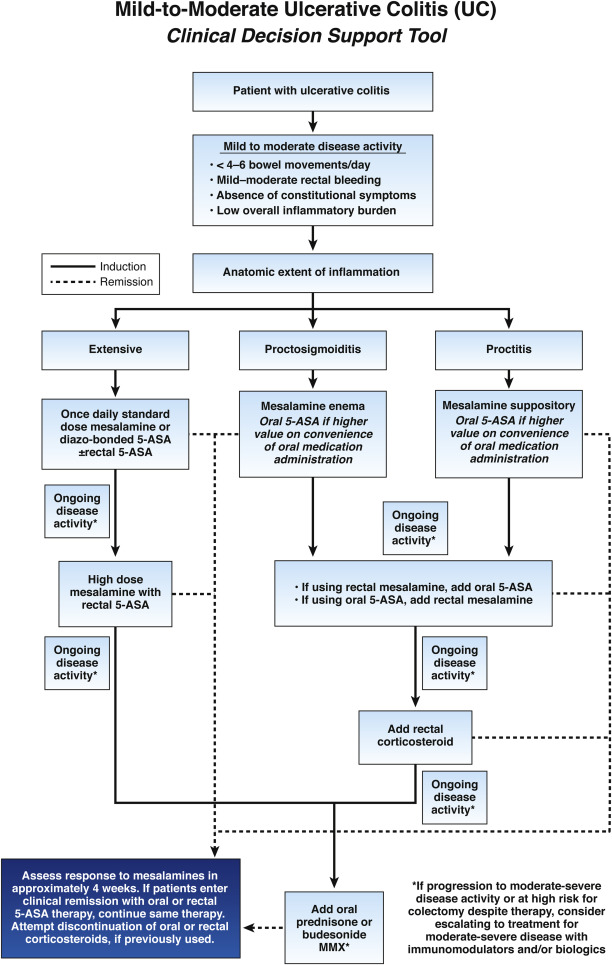
1. In patients with extensive mild–moderate ulcerative colitis (UC), AGA recommends using either standard-dose mesalamine (2–3 g/d) or diazo-bonded 5-aminosalicylates (5-ASA) rather than low-dose mesalamine, sulfasalazine, or no treatment.
2. In patients with extensive or left-sided mild–moderate UC, AGA suggests adding rectal mesalamine to oral 5-ASA.
3. In patients with mild–moderate UC with suboptimal response to standard-dose mesalamine or diazo-bonded 5-ASA or with moderate disease activity, AGA suggests using high-dose mesalamine (>3 g/d) with rectal mesalamine.
4. In patients with mild–moderate UC being treated with oral mesalamine, AGA suggests using once-daily dosing rather than multiple times per day dosing.
5. In patients with mild–moderate UC, AGA suggests using standard-dose oral mesalamine or diazo-bonded 5-ASA, rather than budesonide MMX or controlled ileal release budesonide for induction of remission.
6. In patients with left-sided mild–moderate ulcerative proctosigmoiditis or proctitis, AGA suggests using mesalamine enemas (or suppositories) rather than oral mesalamine.
7. In patients with mild–moderate ulcerative proctosigmoiditis who choose rectal therapy over oral therapy, AGA suggests using mesalamine enemas rather than rectal corticosteroids.
8. In patients with mild–moderate ulcerative proctitis who choose rectal therapy over oral therapy, AGA recommends using mesalamine suppositories.
9. In patients with mild–moderate ulcerative proctosigmoiditis or proctitis being treated with rectal therapy who are intolerant of or refractory to mesalamine suppositories, AGA suggests using rectal corticosteroid therapy rather than no therapy for induction of remission.
10. In patients with mild–moderate UC refractory to optimized oral and rectal 5-ASA, regardless of disease extent, AGA suggests adding either oral prednisone or budesonide MMX.
11. In patients with mild–moderate UC, AGA makes no recommendation for use of probiotics.
12. In patients with mild–moderate UC despite 5-ASA therapy, AGA makes no recommendation for use of curcumin.
13. In patients with mild–moderate UC without Clostridium difficile infection, AGA recommends fecal microbiota transplantation be performed only in the context of a clinical trial.