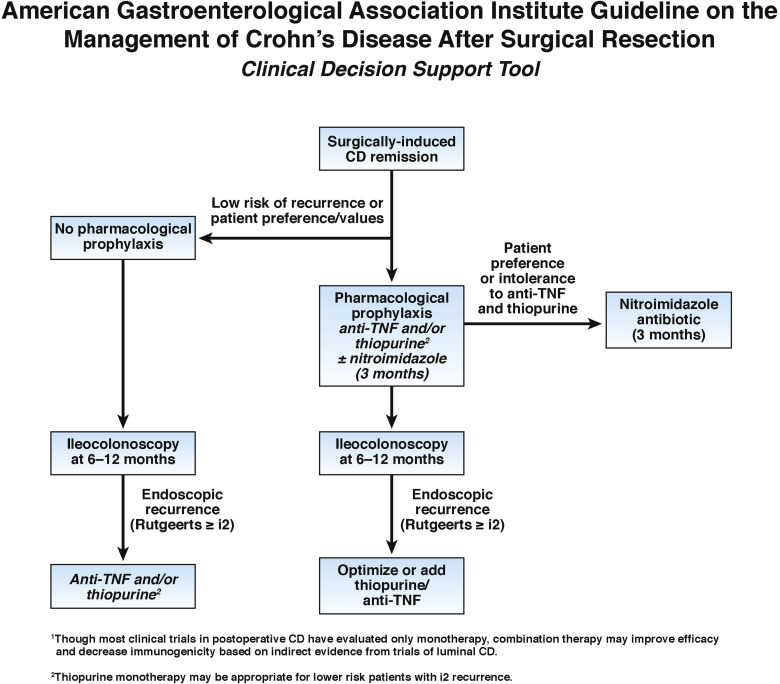
1. In patients with surgically induced remission of Crohn’s disease, AGA suggests early pharmacological prophylaxis over endoscopy-guided pharmacological treatment.
2. In patients with surgically induced remission of Crohn’s disease, AGA suggests using anti-tumor necrosis factor (anti-TNF) therapy and/or thiopurines over other agents.
3. In patients with surgically induced remission of Crohn’s disease, AGA suggests against using mesalamine (or other 5-aminosalicylates), budesonide or probiotics.
4. In patients with surgically induced remission of Crohn’s disease receiving pharmacological prophylaxis, AGA suggests postoperative endoscopic monitoring at 6 to 12 months after surgical resection over no monitoring.
5. In patients with surgically induced remission of Crohn’s disease not receiving pharmacological prophylaxis, AGA recommends postoperative endoscopic monitoring at 6 to 12 months after surgical resection over no monitoring.
6. In patients with surgically induced remission of Crohn’s disease with asymptomatic endoscopic recurrence, AGA suggests initiating or optimizing anti-TNF and/or thiopurine therapy over continued monitoring alone.