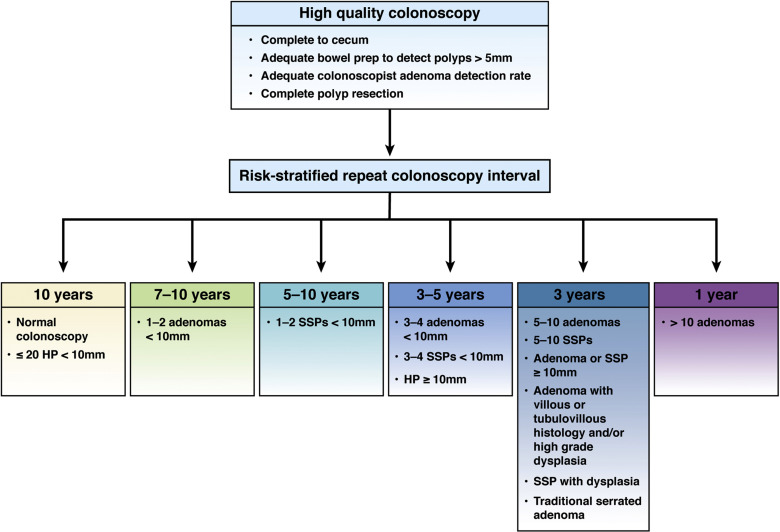
1. For patients with normal, high-quality colonoscopy, repeat colorectal cancer (CRC) screening in 10 years.
2. For patients with 1-2 tubular adenomas <10 mm in size completely removed at a high-quality examination, repeat colonoscopy in 7-10 years.
3. For patients with 3-4 tubular adenomas <10 mm in size completely removed at a high-quality examination, repeat colonoscopy in 3-5 years.
4. For patients with 5-10 tubular adenomas <10 mm in size completely removed at a high-quality examination, repeat colonoscopy in 3 years.
5. For patients with 1 or more adenomas ≥10 mm in size completely removed at high-quality examination, repeat colonoscopy in 3 years.
6. For patients with adenoma containing villous histology completely removed at high-quality examination, repeat colonoscopy in 3 years.
7. For patients with adenoma containing high-grade dysplasia completely removed at high-quality examination, repeat colonoscopy in 3 years.
8. For patients with >10 adenomas completely removed at high-quality examination, repeat colonoscopy in 1 year.
9. For patients with ≤ 20 hyperplastic polyps (HPs) <10 mm in size in the rectum or sigmoid colon removed at a high-quality examination, repeat CRC screening in 10 years.
10. For patients with ≤ 20 HPs <10 mm in size proximal to the sigmoid colon removed at a high-quality examination, repeat colonoscopy in 10 years.
11. For patients with 1-2 sessile serrated polyps (SSPs) <10 mm in size completely removed at high-quality examination, repeat colonoscopy in 5-10 years.
12. For patients with traditional serrated adenomas (TSAs) completely removed at a high-quality examination, repeat colonoscopy in 3 years.
13. For patients with 3-4 SSPs <10 mm at high-quality examination, repeat colonoscopy in 3-5 years.
14. For patients with any combination of 5-10 SSPs <10 mm at high-quality examination, repeat colonoscopy in 3 years.
15. For patients with SSP ≥10 mm at a high-quality examination, repeat colonoscopy in 3 years.
16. For patients with HP ≥10 mm, repeat colonoscopy in 3-5 years. A 3-year follow-up interval is favored if concern about pathologist consistency in distinguishing SSPs from HPs, quality of bowel preparation, or complete polyp excision, whereas a 5-year interval is favored if low concerns for consistency in distinguishing between SSP and HP by the pathologist, adequate bowel preparation, and confident complete polyp excision.
17. For patients with SSP containing dysplasia at a high-quality examination, repeat colonoscopy in 3 years.
18. For patients with history of baseline adenoma removal and one subsequent colonoscopy, recommendations for subsequent surveillance should take into account findings at baseline and first surveillance.
19. For patients with piecemeal resection of adenoma or SSP >20 mm, repeat colonoscopy in 6 months.