1. If feasible, discontinue medications that can cause constipation before further testing.
2. A careful digital rectal examination that includes assessment of pelvic floor motion during simulated evacuation is preferable to a cursory examination without these maneuvers and should be performed before referral for anorectal manometry. However, a normal digital rectal examination does not exclude defecatory disorders.
3. In the absence of other symptoms and signs, only a complete blood cell count is necessary.
4. Unless other clinical features warrant otherwise, metabolic tests (glucose, calcium, sensitive thyroid-stimulating hormone) are not recommended for chronic constipation.
5. A colonoscopy should not be performed in patients without alarm features (eg, blood in stools, anemia, weight loss) unless age-appropriate colon cancer screening has not been performed.
6. Anorectal manometry and a rectal balloon expulsion should be performed in patients who fail to respond to laxatives.
7. Defecography should not be performed before anorectal manometry and a rectal balloon expulsion test.
8. Defecography should be considered when results of anorectal manometry and rectal balloon expulsion are inconclusive for defecatory disorders.
9. Colonic transit should be evaluated if anorectal test results do not show a defecatory disorder or if symptoms persist despite treatment of a defecatory disorder.
10. After discontinuing medications that can cause constipation and performing blood and other tests as guided by clinical features, a therapeutic trial (ie, fiber supplementation and/or osmotic or stimulant laxatives) is recommended before anorectal testing.
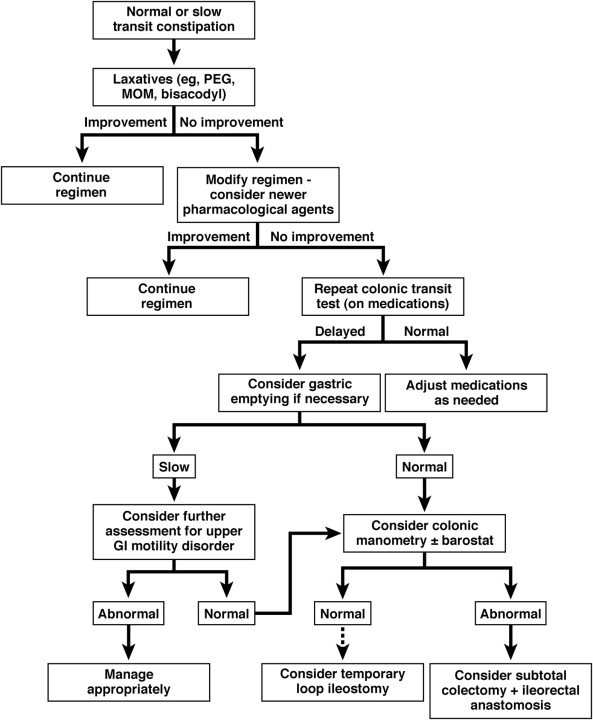
11. Normal transit constipation (NTC) and slow transit constipation (STC) can be safely managed with long-term use of laxatives.
12. Anorectal tests should be performed in patients who do not respond to these measures.
13. Pelvic floor retraining by biofeedback therapy rather than laxatives is recommended for defecatory disorders.
14. When bowel symptoms are refractory to simple laxatives, newer agents should be considered in patients with NTC or STC.
15. Anorectal tests and colonic transit should be reevaluated when symptoms persist despite an adequate trial of biofeedback therapy.
16. A subtotal colectomy rather than continuing therapy with chronic laxatives should be considered for patients with symptomatic STC without a defecatory disorder.
17. Colonic intraluminal testing (manometry, barostat) should be considered to document colonic motor dysfunction before colectomy.
18. Suppositories or enemas rather than oral laxatives alone should be considered in patients with refractory pelvic floor dysfunction.