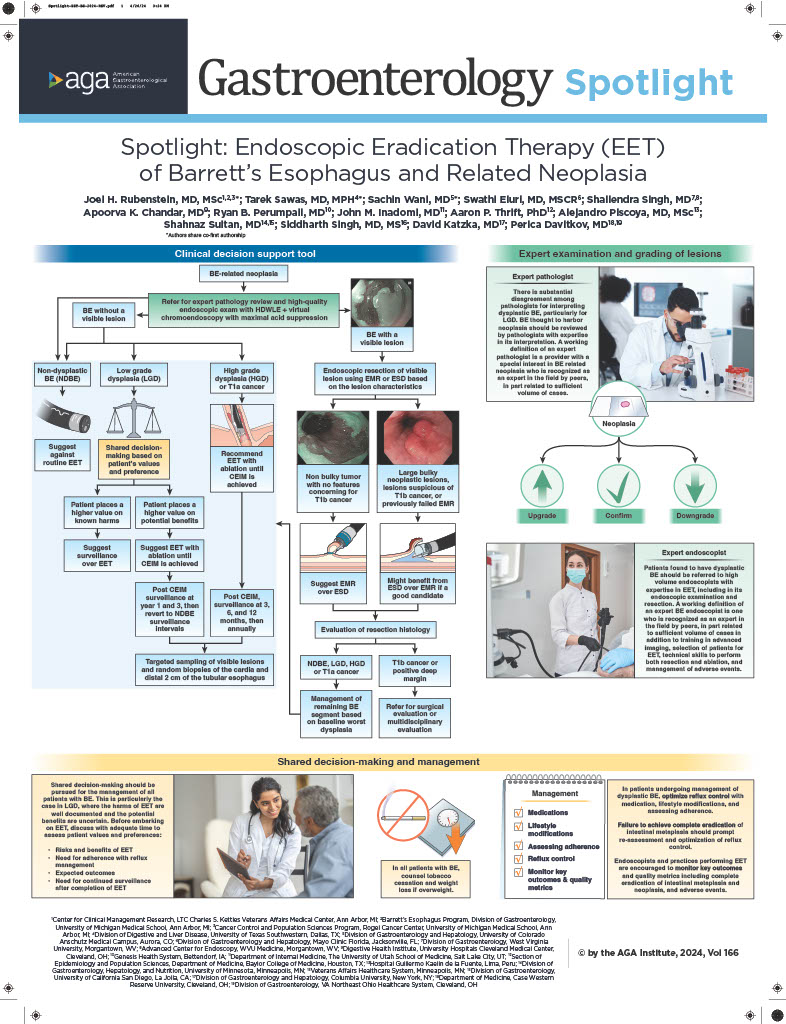
1. In individuals with Barrett’s esophagus (BE) with high-grade dysplasia, AGA recommends endoscopic eradication therapy (EET) over surveillance.
2. In individuals with BE with low-grade dysplasia, AGA suggests EET over surveillance. Patients who place a higher value on the well-defined harms and lower value on the benefits (which are uncertain) regarding reduction of esophageal cancer mortality would reasonably select surveillance endoscopy.
3. In individuals with non-dysplastic BE, AGA suggests against the routine use of EET.
4. In patients undergoing EET, AGA suggests resection of visible lesions followed by ablation of the remaining BE segment over resection of the entire BE segment.
5. In individuals with BE with visible neoplastic lesions that are undergoing endoscopic resection, AGA suggests the use of either endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD) based on lesion characteristics.