1. Women aged 15-50 years with unexplained, recurrent severe abdominal pain without a clear etiology after an initial workup should be considered for screening for an acute hepatic porphyrias (AHP).
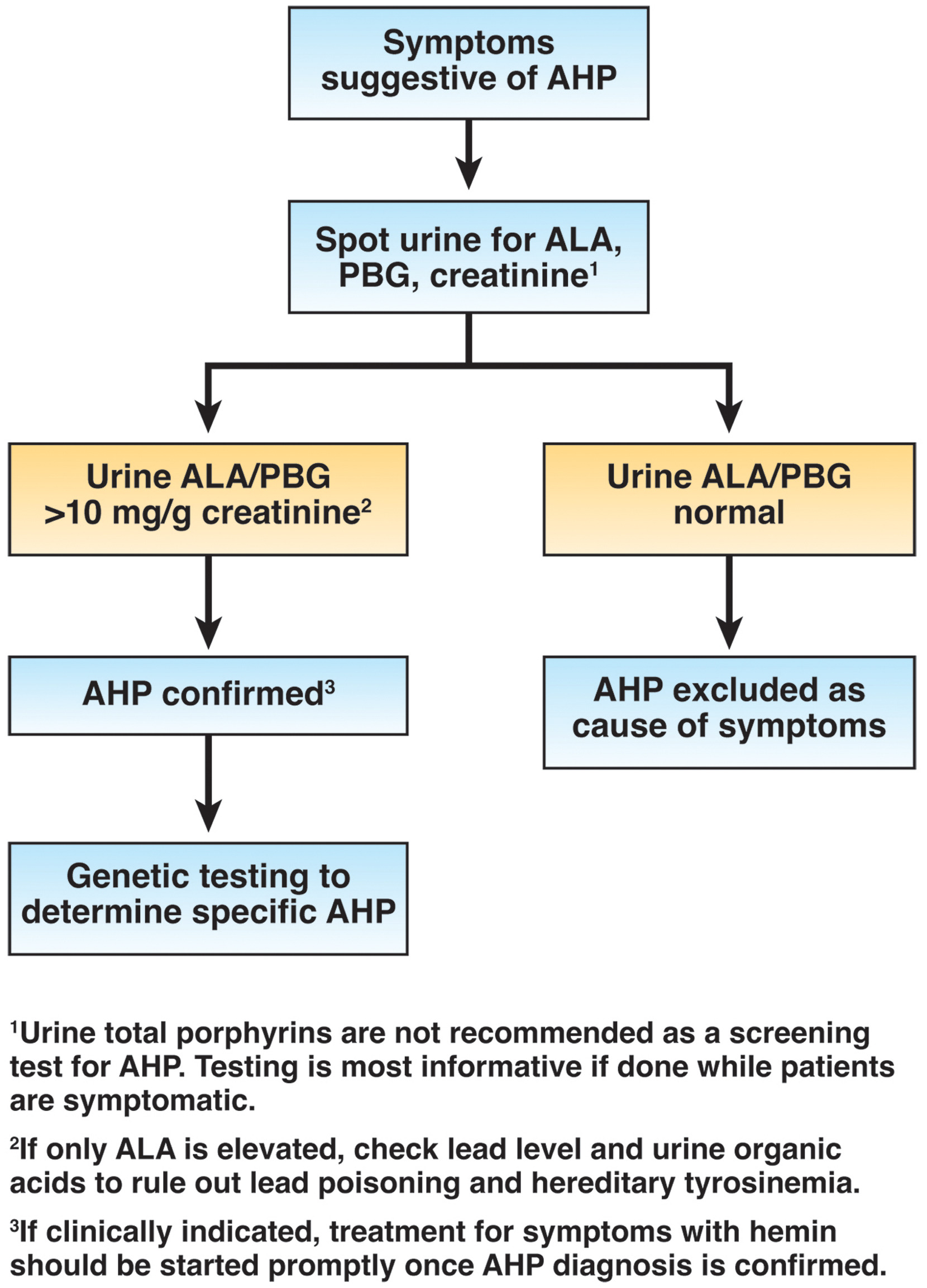
2. Initial diagnosis of AHP should be made by biochemical testing measuring δ-aminolevulinic acid, porphobilinogen, and creatinine on a random urine sample.
3. Genetic testing should be used to confirm the diagnosis of AHP in patients with positive biochemical testing.
4. Acute attacks of AHP that are severe enough to require hospital admission should be treated with intravenous hemin, given daily, preferably into a high-flow central vein.
5. In addition to intravenous hemin, management of acute attacks of AHP should include pain control, antiemetics, management of systemic arterial hypertension, tachycardia, hyponatremia and hypomagnesemia, if present.
6. Patients should be counseled to avoid identifiable triggers that may precipitate acute attacks, such as alcohol and porphyrinogenic medications.
7. Prophylactic heme therapy or givosiran, administered in an outpatient setting, should be considered in patients with recurrent attacks (4 or more per year).
8. Liver transplantation for AHP should be limited to patients with intractable symptoms and significantly decreased quality of life who are refractory to pharmacotherapy.
9. Patients with AHP should be monitored annually for liver disease.
10. Patients with AHP, regardless of the severity of symptoms, should undergo surveillance for hepatocellular carcinoma, beginning at age 50 years, with liver ultrasound every 6 months.
11. Patients with AHP on treatment should undergo surveillance for chronic kidney disease annually with serum creatinine and estimated glomerular filtration rate.
12. Patients should be counseled on the chronic and long-term complications of AHP, including neuropathy, chronic kidney disease, hypertension, hepatocellular carcinoma and the need for long-term monitoring.