NAFLD/NASH screening steps
Step 1: Identifying patients with clinically significant hepatic fibrosis (fibrosis stage 2 or higher) is important for targeted efforts at preventing disease progression. These groups include patients with type 2 diabetes, patients with two or more metabolic risk factors, and those with incidental findings of hepatic steatosis or elevated amino transferases.
Step 2: All at-risk patients identified in Step 1 should be screened for alcohol use and undergo liver function tests (or comprehensive metabolic panel, if done as part of routine care) and a complete blood count as part of the initial screening process.
Step 3: All individuals in the target risk groups should undergo non-invasive testing for clinically significant liver fibrosis using simple, non-proprietary fibrosis scores.
Step 4: Patients with discordant or indeterminate liver stiffness measurement (LSM) results (8.0 to 12.0 kPa) in primary care and endocrine clinics should be referred to hepatology where they may need to undergo either a liver biopsy or magnetic resonance elastography (MRE) for further diagnostic evaluation.
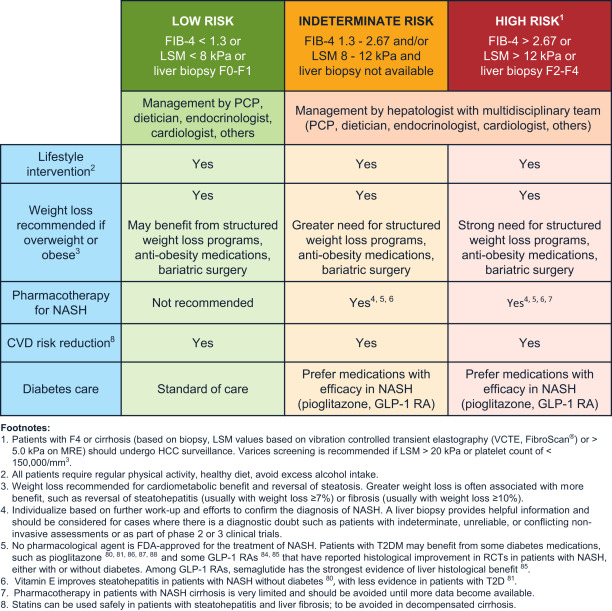
Management of NAFLD/NASH
A multidisciplinary team, including a primary care provider, an endocrinologist for patients with diabetes, and a gastroenterologist/hepatologist, is needed to successfully manage the complexity of care posed by high-risk patients due to obesity, diabetes, CVD and NALFD with fibrosis. The primary goal of screening these patients is to implement early interventions to prevent the development of cirrhosis and liver-related and all-cause mortality. Providers must also try to help patients reverse the unfavorable metabolic profile as CVD is the primary cause of morbidity and mortality in patients with NAFLD/NASH before the development of cirrhosis. In all risk groups, appropriate physician-patient communication should guide shared decision-making.
Patients at low-risk of advanced fibrosis should be managed using therapeutic lifestyle interventions, such as weight loss, as appropriate, nutritional strategies, stress management, regular physical exercise and avoiding excess alcohol intake. Specific pharmacological treatment targeting liver steatosis is not necessary in this lower-risk population.
Patients at high-risk advanced fibrosis should be managed by a multidisciplinary team closely coordinated by a hepatologist who can monitor for cirrhosis, hepatocellular carcinoma and other cirrhosis-related complications. In these patients, we recommend aggressive lifestyle changes aimed at long-term weight loss, including a greater use of formal weight loss programs and potentially, surgery.
Patients at indeterminate-risk of advanced fibrosis should be managed using a similar approach to high-risk patients, along with further work-up and efforts to confirm the stage of hepatic fibrosis. In some cases, proprietary plasma biomarker tests for fibrosis staging or additional imaging-based fibrosis measurement (i.e., MRE) studies may be used to guide patient care.